Contributed by Nick Gordon (@Ngordon)
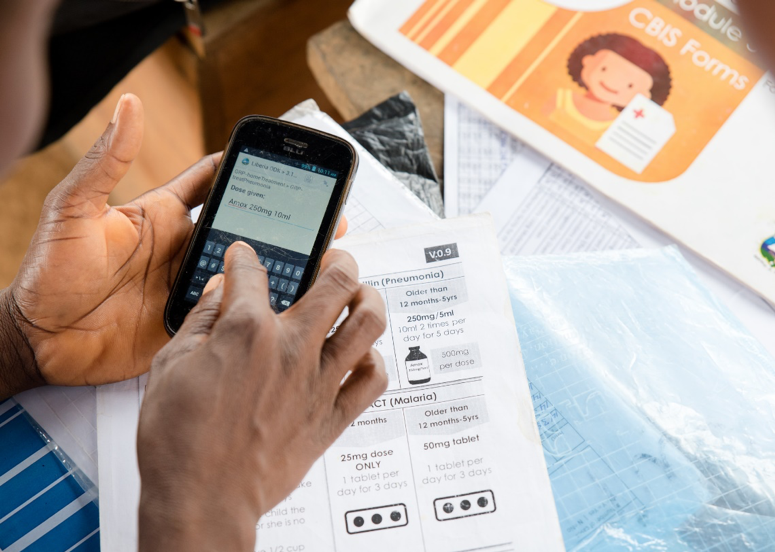
A Liberia Community Health Assistant uses ODK to collect to collect information and guide decision making while diagnosing and treating sick children.
Project URL: http://lastmilehealth.org
What is the organization responsible for the ODK project? What sort of work do they do? What is your role?
Last Mile Health (LMH). Founded in Liberia in 2007, Last Mile Health partners with governments to design, scale, and advocate for national networks of professional community health workers (CHWs) who strengthen health systems and save lives at the last mile. I’ve worked with the organization for four years and act as the Digital Health Lead. I help set the strategy and direction for the Digital Health Department, which supports governments apply technology solutions to their health programs.
What is the goal of the project?
To provide Liberia’s Community Health Assistant Program with an electronic data collection platform that functions in a fully offline environment. The project equips CHWs with tools to collect data and more accurately diagnose and treat sick children and transfer data without internet connection.
How many people are involved in the project? How many enumerators or field data collectors?
This project was originally housed within LMH’s Research, Monitoring & Evaluation Department. It is now being managed by a 5-person Digital Health Team. All software development has been managed by external contractors. Since 2015, the RM&E Department has also used Liberia ODK to conduct surveys and GIS mapping in remote regions of Liberia.
It is currently being used by 380 CHWs and nurse supervisors. Last Mile Health is supporting the Government of Liberia to digitize data collection and reporting tools across the national Community Health Assistant Program with approximately 4,000 users in 2019.
What is/are the geographical region(s) where ODK is being used?
The initiative is used in remote Liberia (all communities >5km from a health facility). The terrain and environment are particularly challenging, and our end users often have no electricity or network connectivity. Even when there is network access, network speeds are often insufficient to reliably transfer data – particularly, audio, video, and image content.
What is the time frame of the project (eg days, weeks, years), or what determines when the project will be done?
The project began in January 2015 as a data collection tool to screen patients for Ebola. Since then, more functionality and forms have been added and it has been scaled to 380 health workers. LMH is now supporting the Liberia Ministry of Health to scale the initiative nationally. Our organization and department seek to apply and iterate on sustainable technologies by designing with government ownership and scalability in mind. Though the underlying technology may change, the initiative is planned to run indefinitely.
What ODK tools do you use and which features are most useful to your project?
In this project, we have only used this modified version of ODK Collect. The most useful “feature” of this technology has undoubtedly been this active ODK community, which has made it easy for us to get this up and running from scratch.
The project has seen the following modifications to ODK (available on github):
-
LODK 1.0: In the first round of modifications, we modified ODK Collect to transfer completed forms and new form packages between devices over Bluetooth.
-
LODK 2.0: We modified ODK Collect to set roles depending on the user. This allowed us to consolidate form package updates into a single file while having ODK only display relevant forms to the user.
-
LODK 3.0: We modified ODK with “auto archiving”, which stored completed forms locally on the device even after data transfer. In the instance that data was lost while being transferred between users, data from the originating device could be re-transferred over Bluetooth.
-
LODK 4.0: We modified ODK to have case management functions and summary data reports. Case management added a new interface to view detailed information on client visits, which allows users to review, follow-up on, and close. Summary statistics allowed administrators to configure forms to summarize information from completed forms. For example, # of children treated in last 7 days, # of sick children needing follow-up, etc. It breaks my heart, but we don’t currently have the capacity to support this version. However, I still plan on fixing some minor bugs and developing documentation.
What other non-ODK software do you use that might be of interest to the ODK community?
We use a couple of tools that people might like:
-
We do all of our form development in CommCare HQ. I’m in love with this form designer, and it keeps getting better each year. We extract XML code from the tool, run a few small macros to make it usable by Collect, and then consolidate all forms into a single XML document.
-
We created a custom kiosk software called Palm Kiosk. This tool locks down mobile phones so that the user is restricted to applications approved by a device administrator. We use this for data security, to better control program fidelity, and to reserve battery life for health applications.
-
Last Mile Health partnered with Digital Campus to deploy their eLearning app, Oppia Mobile. It has been customized with similar Bluetooth transfer capabilities and has the ability to send/receive multimedia training content in offline contexts. This is part of a growing ecosystem of training applications being designed under an initiative called the Community Health Academy.
Can you give an overview of what the regular daily/weekly schedule is for your project? How do you go about acquiring, transmitting and analyzing your data? etc.
Mobile phones with Liberia ODK installed are deployed to remote Liberian communities, where it is used to collect information on health worker activities and guide clinical practices. During bi-monthly supervision visits, nurse supervisors use the platform to transfer the CHWs data over Bluetooth to his or her phone. In the reverse direction – supervisors can also send updated form packages to CHWs. Data is uploaded via a custom web app and sent to a SQL database. Data is maintained and analyzed by LMH’s Research, Monitoring & Evaluation team. In upcoming deployments of the initiative, data systems will be modified to directly integrate with Liberia’s central database and reporting systems.
What have been the greatest successes in your project?
Increasing the sheer amount of data collected in our directly implemented network. Related paper-based data systems collect 44 data elements on a monthly-basis, which are aggregated in sets of 10 users. Through ODK, we now collect hundreds of different data elements and can disaggregate program data at the patient-interaction level. This allows for much more complex evaluations and a more nuanced understanding of the program.
What are the biggest technical and/or logistical challenges in the project?
Logistically, the greatest challenge has been Liberia’s challenging terrain, which makes it difficult to collect data from remote areas with low population density. These areas have little access to reliable cellular networks, which has been the primary drive behind designing connectivity solutions around Bluetooth rather than cellular networks. Half of the year also sees heavy rainfall, which makes charging via solar solutions and capturing GIS coordinates difficult.
From a technical standpoint, the biggest limitation of ODK has been the user interface and generating reports at the field-level. As a survey tool, it is flexible and reliable. However, as a health technology, it has been challenging to optimize the user experience for complex workflows such as restock, case management, and supervision. Right now, I’m excited to start getting to know ODK2 tools a bit better. I am hopeful that its easily customizable UX will be able to build a more user-friendly experience.

Digital Health Operator, Washington Gbowoe, navigates challenging road conditions to conduct data collection in Grand Gedeh County.

Supervisor, Markson Farley transfers completed forms from a Community Health Assistant’s (Zarkpa Yeoh) phone to his own phone over Bluetooth.

The Digital Health Team setting up thousands of mobile phones to create an “out-of-the-box” digital health deployment experience for the Liberia Ministry of Health.

The Digital Health Team in Liberia supports the Ministry of Health to develop and deploy fit-for-purpose technologies to healthcare delivery.